
Subscribe to our newsletter and get your FREE guide,
Natural Back Pain Relief: 16 Choices for Lasting Comfort.
If a patient suffering from chronic joint pain due to arthritis opts to have a joint replacement surgery, the orthopedic surgeon will replace the existing joint surfaces with artificial joint prostheses. These prostheses, or prosthetic components, must adhere to the patient's natural bone. How this adhesion is achieved depends on the type of prosthesis used:
- A cemented joint prosthesis uses fast-drying bone cement to help affix it to the bone.
- A cementless joint prosthesis, sometimes called a press-fit prosthesis, is specially textured to allow the bone to grow onto it and adhere to it over time.
An important factor to consider when deciding on joint replacement is cement vs. cementless prosthetics.
Before a knee replacement, hip replacement, shoulder replacement, or other joint replacement surgery, the surgeon will talk to the patient and decide whether to use cemented prostheses, cementless prostheses, or a combination of the two. The type of component(s) used may depend on the patient's physiology, the type of surgery being done, and the surgeon's preference.
See Orthopedic Surgeon for Arthritis Treatment
The pros and cons of each type of prosthesis are described below.
advertisement
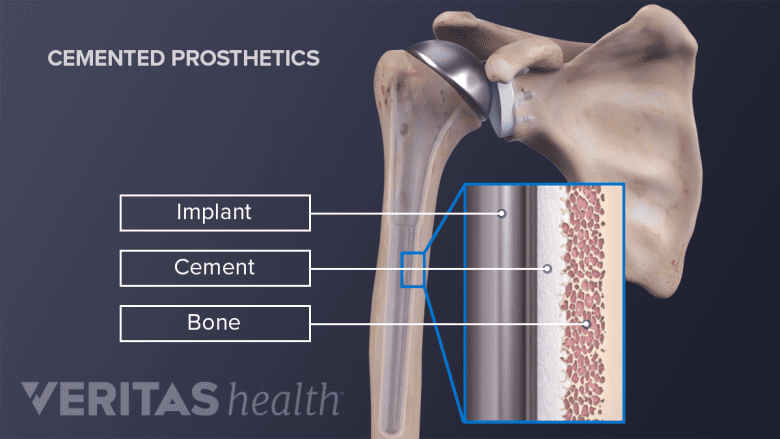
Cemented Joint Prostheses: Advantages and Disadvantages
A cemented prosthesis is designed to have a layer of bone cement, typically an acrylic polymer called polymethylmethacrylate (PMMA), in between the patient's natural bone and the prosthetic joint component.
There are a few advantages to using bone cement in joint replacement surgeries:
- Bone cement allows a surgeon to affix prosthetic joint components to a bone that is slightly porous from osteoporosis.
- A small amount of antibiotic material can be added to the bone cement, helping to decrease the risk of post-surgical infection.
- The bone cement dries within 10 minutes of application, so the surgeon and patient can be confident the prosthetic is firmly in place.
The drawback to using bone cement is that it may degrade over time and bits of cement can break off, potentially causing problems:
- A breakdown of the cement can cause the artificial joint to come loose, which may prompt the need for another joint replacement surgery (revision surgery).
- The cement debris can irritate the surrounding soft tissue and cause inflammation.
- While rare, the cement can enter the bloodstream and end up in the lungs, a condition that can be life-threatening. This risk is greatest for people who undergo spinal surgeries.
Exactly how often these complications occur following specific types of joint replacement surgeries is uncertain. Not all patients with bone cement debris experience symptoms. Bits of cement debris can be removed arthroscopically to alleviate or prevent symptoms.
In rare cases, patients have an allergic reaction to the bone cement and must undergo a second surgery to remove the glue and prostheses.
Cementless Joint Prostheses: Advantages and Disadvantages
A cementless prosthesis, also called a press-fit prosthesis, has a rough surface or porous coating that encourages the natural bone to grow onto it. New bone growth will span only 1 or 2 mm, so the surgeon must use special tools to shape the natural bone to fit snugly with the prosthesis.
Some prosthetic components have screws or pegs that help hold the bone and prostheses in place until new bone growth can create a more secure attachment. For example, during some shoulder replacement surgeries, the new shoulder sockets are backed with short pegs that fit into the patients' natural bone, thereby helping to stabilize the new prosthesis and the patient's scapula (shoulder blade).
A number of surgeons prefer cementless components because:
- They believe cementless components offer a better long-term bond between the prostheses and bones.
- Cementless components eliminate worry about the potential breakdown of cement.
The downsides to cementless prostheses are that:
- Press-fit prostheses require healthy bones. Patients with low bone density due to osteoporosis may not be eligible for these components.
- It can take up to three months for bone material to grow into a new joint component.1Arthritis Foundation. "Types of Replacement Parts." Excerpted from All You Need to Know About Joint Surgery. Accessed January 20, 2012. www.arthritis.org.,2National Institute of Arthritis and Musculoskeletal and Skin Diseases. Questions and Answers About Hip Replacement. Updated April 2012. Accessed August 26, 2013. www.niams.nih.gov.
Because it takes time for the natural bone to fully adhere to the new joint components, experts debate whether or not patients should postpone putting their full weight on new joints.
advertisement
How Soon Can A Patient Walk on a Cementless Hip or Knee Prosthesis?
Patients may be advised to avoid full weight-bearing on cementless components during the first 4 to 12 weeks after surgery. Limited partial weight-bearing is allowed. This cautious approach lengthens a patient's rehabilitation schedule but guards against stressing or loosening a new joint, which can be painful and require a second surgery.
Alternatively, other patients may be told to begin putting full body weight on the new joints just a day or two after surgery.3Taunt C, Finn H, Baumann P. Immediate Weight Bearing After Cementless Total Hip Arthroplasty. ORTHOPEDICS. 2008; 31 Studies of cementless hip replacements support this approach, showing that well-fitted cementless hip prostheses can handle the pressure.3Taunt C, Finn H, Baumann P. Immediate Weight Bearing After Cementless Total Hip Arthroplasty. ORTHOPEDICS. 2008; 31,4Hol AM, van Grinsven S, Lucas C, van Susante JL, van Loon CJ. Partial versus unrestricted weight bearing after an uncemented femoral stem in total hip arthroplasty: recommendation of a concise rehabilitation protocol from a systematic review of the literature. Arch Orthop Trauma Surg. 2010 Apr;130(4):547-55. PMID: 20012073.,5Markmiller M, Weiss T, Kreuz P, Rüter A, Konrad G. Partial weightbearing is not necessary after cementless total hip arthroplasty: a two-year prospective randomized study on 100 patients. Int Orthop. 2011 Aug;35(8):1139-43. PMID: 20623280,6Rao RR, Sharkey PF, Hozack WJ, Eng K, Rothman RH. Immediate weightbearing after uncemented total hip arthroplasty. Clin Orthop Relat Res. 1998 Apr;(349):156-62. PubMed PMID: 9584378. Full weight-bearing during early recovery and rehabilitation promotes healthy muscle and bone tissue and lowers the risk of post-surgical deep vein thrombosis (DVT).
Research in this area is ongoing. For now, surgeons must base their rehabilitation recommendations on many factors, such as the joint being replaced, the specific component being used, the patient's physiology, and past experience. Patients who are concerned with this issue should talk to their doctor.
See “When Can I…?” Answers for Knee Replacement Patients
Hybrid Joint Component Solutions
Some knee replacement, hip replacement, shoulder replacement, and other joint replacement surgeries use both cementless and cemented components. For example, some knee replacements use bone cement to affix the tibial (shin bone) and patellar (knee cap) components, while using cementless components on the femur (thigh bone). Early research this method is promising, but more study needs to be done.7American Academy of Orthopeadic Surgeons. "Cemented and Cementless Knee Replacement." Accessed January 31, 2012. orthoinfo.aaos.org.
Future Joint Prosthesis Alternatives
Researchers are continually looking to improve upon existing prosthesis designs as well as methods of affixing prostheses to natural bone. For example, recent research has been done with components made of highly porous metals such as tantalum. Initial studies indicate tantalum may facilitate a strong bond between bone and prosthesis in a relatively short timeframe.8Howard, James L, Jeremy Kudera, David G Lewallen, and Arlen D Hanssen. "Early Results of the Use of Tantalum Femoral Cones for Revision Total Knee Arthroplasty." The Journal of Bone and Joint Surgery. American Volume 93, no. 5 (March 2, 2011): 478–84. doi:10.2106/JBJS.I.01322. This research is still in the very early stages and more clinical study needs to be done.
- 1 Arthritis Foundation. "Types of Replacement Parts." Excerpted from All You Need to Know About Joint Surgery. Accessed January 20, 2012. www.arthritis.org.
- 2 National Institute of Arthritis and Musculoskeletal and Skin Diseases. Questions and Answers About Hip Replacement. Updated April 2012. Accessed August 26, 2013. www.niams.nih.gov.
- 3 Taunt C, Finn H, Baumann P. Immediate Weight Bearing After Cementless Total Hip Arthroplasty. ORTHOPEDICS. 2008; 31
- 4 Hol AM, van Grinsven S, Lucas C, van Susante JL, van Loon CJ. Partial versus unrestricted weight bearing after an uncemented femoral stem in total hip arthroplasty: recommendation of a concise rehabilitation protocol from a systematic review of the literature. Arch Orthop Trauma Surg. 2010 Apr;130(4):547-55. PMID: 20012073.
- 5 Markmiller M, Weiss T, Kreuz P, Rüter A, Konrad G. Partial weightbearing is not necessary after cementless total hip arthroplasty: a two-year prospective randomized study on 100 patients. Int Orthop. 2011 Aug;35(8):1139-43. PMID: 20623280
- 6 Rao RR, Sharkey PF, Hozack WJ, Eng K, Rothman RH. Immediate weightbearing after uncemented total hip arthroplasty. Clin Orthop Relat Res. 1998 Apr;(349):156-62. PubMed PMID: 9584378.
- 7 American Academy of Orthopeadic Surgeons. "Cemented and Cementless Knee Replacement." Accessed January 31, 2012. orthoinfo.aaos.org.
- 8 Howard, James L, Jeremy Kudera, David G Lewallen, and Arlen D Hanssen. "Early Results of the Use of Tantalum Femoral Cones for Revision Total Knee Arthroplasty." The Journal of Bone and Joint Surgery. American Volume 93, no. 5 (March 2, 2011): 478–84. doi:10.2106/JBJS.I.01322.

advertisement